

Translate this page into:
Laparoscopic management of scar ectopic pregnancy
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
This case presentation illustrates correct diagnosis of scar ectopic pregnancy by ultrasonography in correlation with the compliant of intermenstrual bleeding and pain in lower abdomen. The transvaginal ultrasonography finding suggested missed abortion in scar pregnancy. Prompt decision of laparoscopic management was taken depending upon the status of the patient and desire to preserve the fertility. Patient recovered uneventfully and conceived naturally after 10 months. She had uneventful antenatal period, underwent elective lower segment cesarean section (LSCS) at 36 weeks and delivered full-term baby. Early and accurate diagnosis, prompt management of scar ectopic pregnancy can preserve fertility.
Keywords
Cesarean section
laparoscopic management
scar ectopic pregnancy
transvaginal ultrasonography

INTRODUCTION
Cesarean scar pregnancy is the rarest form of ectopic pregnancies with an incidence of 1:1800-1:2216 in women with an ectopic pregnancy and at least one previous cesarean section.[1] In cesarean scar pregnancy, the gestational sac is implanted in the myometrium at the site of a previous cesarean section. Early diagnosis of cesarean scar pregnancy is essential to avoid serious complication such as severe hemorrhage, which may require hysterectomy and endanger the woman's life, and affect negatively on future fertility.[2] Pre-operative confirmation of diagnosis is very difficult and hysterectomy is often required to control bleeding during operation.[3] We report a case of an ectopic gestation in a previous cesarean section scar diagnosed by ultrasound and hysteroscopy, and managed successfully by operative laparoscopy conserving the fertility.
CASE REPORT
A 25-year-old lady, G 2 P 1 A 1 presented in Out Patient Department with complain of intermenstrual bleeding, pain in lower abdomen, general weakness, and dyspareunia since 1 week. She had undergone an uneventful term transverse lower segment cesarean section (LSCS) one yearback and had one previous spontaneous abortion. Uterus was soft, bulky, retroverted, and retroflexed. The urine pregnancy test was positive.
Transvaginal ultrasonography showed single gestational sac in gravid uterus in lower uterine segment at level of previous LSCS scar which suggested scar pregnancy. Fetal heart flicker was absent and chorionic outline of gestational sac was irregular suggesting missed abortion in scar pregnancy. A small right ovarian cyst was also present. The findings fulfilled the proposed sonographic criteria for diagnosis:
An empty uterus,
An empty cervical canal,
On a view of the uterus a discontinuity in the anterior uterine wall when running through the amniotic sac,
The gestational sac is located in the anterior part of the isthmic portion of the uterus with a diminished myometrial layer between the bladder and the sac.[4]
After appropriate counselling with the patient, decision was taken for possible operative laparoscopy treatment. Under general anesthesia, 5 mm trocar introduced into abdomen and pneumoperitoneum was created. Moreover, 3 × 3 cm bulge of scar pregnancy on lower uterine segment was seen. Bladder sound gently passed through urethra to see the extend of bladder. No obvious bladder adhesions were seen. Cervical dilation was done and was easy. Through hysteroscope, gestational sac was seen at scar site on anterior wall [Figure 1]. Rest of the cavity was normal. Gentle suction followed by curettage was done but only few products were separated and removed. Bleeding was increased hence decision of removal of products through laparoscopy was taken. On scar site loose fold of peritoneum was identified and bladder pushed down. After protecting bladder, incision was taken on the scar, and products of conception were removed completely. Thorough lavage of the cavity was done and hemostasis was achieved. Scar sutured with No. 1 vincryl. Bleeding from vagina was checked and no active bleeding was observed. Small cyst on right ovary was identified and punctured. The patient was discharged on the second post-operative day after an uneventful recovery.
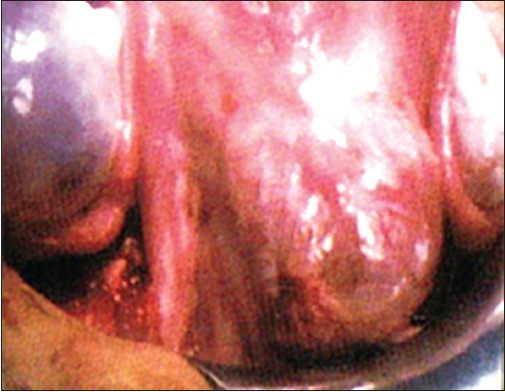
- Scar ectopic pregnancy
Patient conceived naturally after 10 months. She had uneventful antenatal period, underwent elective LSCS at 36 weeks and delivered full-term baby.
DISCUSSION
Even though a rare condition, the incidence of cesarean scar pregnancy is on the rise due to increase in the number of cesarean deliveries and availability of better imaging techniques. The rarity of this type of ectopic pregnancy universally results in the lack of therapeutic protocols on optimal management. The selection of treatment modality is based on severity of symptoms, medical condition of the patient, desire to preserve fertility, gestational age, and surgical experience. Treatment modalities include expectant management, surgical management and medical management. Micheal A. Rotas et al., reported a review of 112 cases on the clinical presentation, diagnosis, and treatment modalities of cesarean scar ectopic pregnancy. Various treatments provided to 112 women included expectant management, laparotomy, laparoscopy, hysteroscopy, dilation and curettage, selective uterine artery embolization, systemic methotrexate, local methotrexate, combined methotrexate, local embryocides, and sac aspiration.[6] It is observed that most of the treatment options may lead to complications ranging from bleeding to uterine rupture that necessitated additional therapy like hysterectomy. Methotrexate therapy is most commonly recommended for scar ectopic pregnancy but contraindicated in case of severe or persistent abdominal pain.[5] Micheal A. Rotas et al., concluded laparoscopic approach to be reasonable as long as the appropriate expertise and facilities are available. In the case presented, the condition is managed by laparoscopic resection of the scar pregnancy and securing the defect. The laparoscopic management even fulfilled the criteria to optimally preserve the fertility of the patient. Thus, in case of scar ectopic pregnancy with symptoms of intermenstrual bleeding, pain in lower abdomen, general weakness, and dyspareunia, it should be managed laparoscopically without delay to avoid complications like bleeding, uterine rupture that may lead to hysterectomy hampering the fertility of the patient.
CONCLUSION
It is important that early and accurate diagnosis and treatment is obtained in order to avoid complications and preserve fertility in cases of scar ectopic pregnancy.
Source of Support:
Nil
Conflict of Interest:
None declared.
REFERENCES
- Cesarean scar pregnancies successfully treated with methotrexate. Acta Obstet Gynecol Scand. 2009;88:720-3.
- [Google Scholar]
- Ectopic intramural pregnancy developing at the site of a cesarean section scar: A case report. Cases J. 2009;2:9404.
- [Google Scholar]
- Laparoscopic management of an ectopic pregnancy in a previous Caesarean section scar. Hum Reprod. 1999;14:1234-6.
- [Google Scholar]
- Medical treatment of ectopic pregnancy: A committee opinion. Fertil Steril. 2013;100:638-44.
- [Google Scholar]
- Caesarean scar ectopic pregnancies: Etiology, diagnosis and management. Obstet Gynaecol. 2006;107:1373-81.
- [Google Scholar]




