

Translate this page into:
A rare case of OHVIRA in an adolescent presenting with dysmenorrhea: A case report
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
This article was originally published by Wolters Kluwer - Medknow and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Here we present a rare case of complex uterine anomaly with Obstructed Hemivagina and ipsilateral renal agenesis (OHVIRA), also known as the Herlyn-Werner-Wunderlich syndrome (HWWS). A 16-year-old girl presenting with dysmenorrhea underwent ultrasonography, intravenous urogram (IVU), and magnetic resonance imaging (MRI) of kidney, ureter, and bladder (KUB). An abdominopelvic MRI was found to be very effective in reaching appropriate diagnosis with the avoidance of interventions like laparoscopy or laparotomy, which was needed in the past to diagnose this rare anomaly. We also discuss the embryopathogenesis of this anomaly and review the literature.
Keywords
Herlyn-Werner-Wunderlich syndrome (HWWS)
mullerian and mesonephric anomalies
obstructed hemivagina
ipsilateral renal agenesis (OHVIRA) syndrome
unilateral renal agenesis

INTRODUCTION
Obstructed hemivagina and ipsilateral renal agenesis (OHVIRA), or Herlyn-Werner-Wunderlich syndrome (HWWS), are rare congenital mullerian and mesonephric anomalies with a characteristic triad of uterine didelphys, unilateral obstructed hemivagina, and ipsilateral renal agenesis. Patients with this anomaly usually present after menarche with dysmenorrhea, pelvic pain, and a mass. Nonspecific symptoms like pelvic pain or dysmenorrhea in the pubertal age group lead to delay in the diagnosis of this condition. Therefore, strong suspicion and knowledge of this anomaly are essential for a precise diagnosis. Delay in diagnosis may cause the development of pelvic endometriosis, pyohematocolpos, pyohematometra, pyosalpinx, and pelvic adhesions leading to primary infertility that may result in marital disharmony and worsen the socioeconomic status.[1] Magnetic resonance imaging (MRI) is the modality of choice for the diagnosis of HWWS and other such anomalies because of better anatomic delineation of pelvic structures and higher sensitivity to blood products.
CASE REPORT
A 16-year-old girl attended the Gynecology Outpatient Department (OPD) of Medical College, Kolkata, West Bengal with the complaint of dysmenorrhea since menarche. She had attained menarche at the age of 13 years. She was otherwise healthy without any other significant complaint. Her clinical examination, including abdominal examination, was unremarkable. She was advised ultrasonographic evaluation of the pelvis. Ultrasonography (USG) revealed two separate uteri and cervix. An echogenic collection was seen in the vagina [Figure 1]. Incidentally, it was also found that the left kidney was absent in its normal anatomical location [Figure 2].

- Trans abdominal USG transverse view shows bicornuate uterus sagital view showing an echogenic collection within the vagina

- Trans abdominal USG left oblique coronal view showing normal spleen and nonvisualization of left kidney in the renal fossa. Digital IVU after 40 min of contrast administration shows normal excretion of contrast through the right kidney, pelvicalyceal system, and ureter and nonvisualization of the left kidney, pelvicalyceal system, and ureter
Based on these findings, she was further advised an intravenous urogram (IVU) to exclude the hidden ectopic left kidney. Her IVU revealed normal excretion of contrast through the right kidney while the left kidney was not visualized [Figure 2].
Subsequently, pelvic MRI with magnetic resonance (MR) urography was considered for precise delineation of the anomaly. The MRI of the patient revealed two separate uteri, two cervix and two vagina with collection in left vagina. Left vaginal collection showed hypointense signal on both T1 - and T2 - weighted images, which was suggestive of blood products. MR urogram revealed the same findings as IVU [Figures 3 and 4].
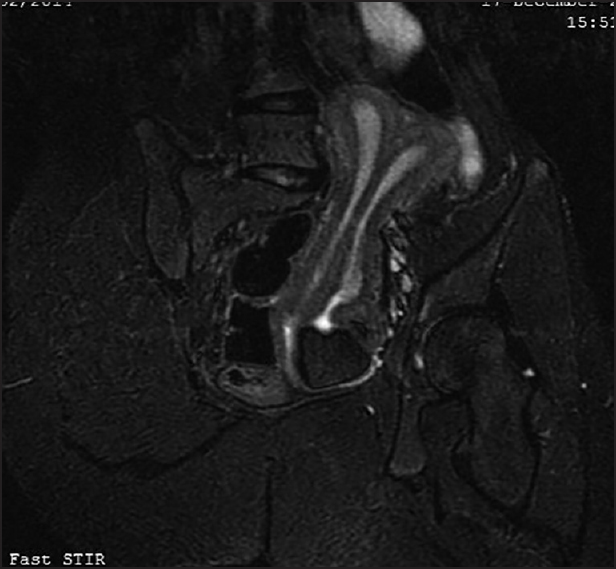
- Pelvic MRI coronal view showing uterine didelphys and left obstructed hemivagina with hematocolpos

- Abdominopelvic MRI and MR urogram showing normal kidney, pelvicalyceal system and ureter on right side with non-visualization of left kidney, pelvicalyceal system and ureter
On the basis of the above mentioned findings, a diagnosis of uterine didelphys with obstructed left vagina was considered. As the patient was also having ipsilateral renal agenesis a final diagnosis of HWWS or OHVIRA was done. The patient is now on oral medications for symptomatic relief. Surgical excision of the vaginal septum has been planned.
DISCUSSION
Among women, the overall prevalence of mullerian duct anomaly is 2-3%.[2] The incidence of uterine didelphys related to HWW is approximately 1/2,000 to 1/28,000 and it is accompanied by unilateral renal agenesis in 43% of the cases. The incidence of unilateral renal agenesis is 1/1,100 and 25-50% of affected women exhibit associated genital abnormalities. Renal tract anomalies are associated with mullerian duct anomalies in 30% of the cases.
The mullerian duct anomaly classification is a seven point system proposed by the American Fertility Society that can be used to describe a number of embryonic mullerian duct anomalies.[3]
Class I: Uterine agenesis/uterine hypoplasia
Class II: Unicornuate uterus/unicornis unicollis, ~6-25%
Class III: Uterus didelphys, ~5-11%
Class IV: Bicornuate uterus: ~10-39%
Class V: Septate uterus: commonest anomaly, ~34-55%
Class VI: Arcuate uterus, ~7%
Class VII: In utero diethylstilbestrol (DES) exposure: T-shaped uterus
According to the abovementioned classification, our case belonged to Class III.
The syndrome of obstructed hemivagina and ipsilateral renal anomaly was initially reported in 1922 and is known as HWWS or more recently, by the acronym OHVIRA.[1,4,5,6] The incidence of uterine didelphys related to OHVIRA is approximately 1/2,000 to 1/28,000 and it is accompanied by unilateral renal agenesis in 43% of cases.[5] The OHVIRA syndrome classically occurs in the setting of uterine didelphys and more rarely, in a septate uterus.[2,3] Renal agenesis is the most commonly reported urologic anomaly in OHVIRA syndrome although other malformations, like renal duplication and multicystic dysplastic kidney, have also been reprted.[3]
Embryopathogenesis of OHVIRA starts at around 8 weeks of gestation, simultaneously affecting both mullerian and metanephric ducts. Renal agenesis is thought to be due to growth arrest in one of the wolfian ducts. This, in turn, affects the position of ipsilateral mullerian duct. The malpositioned mullerian duct cannot undergo successful fusion, thereby resulting in uterus didelphis.[7] Haddad et al. studied the associations of blind hemivagina in 42 patients and found that it was associated with renal agenesis in almost all the patients. In addition, blind hemivagina with ipsilateral renal agenesis was generally associated with uterus didelphys; however, rare cases of septate uterus were also found.[3]
The typical patient with this rare condition usually presents after menarche with nonspecific symptoms of recurrent pelvic pain or dysmenorrhea from progressive distention of the obstructed hemivagina. Early and accurate diagnosis is important because early therapeutic intervention can relieve symptoms and prevent complications related to chronic obstructions, e.g., hematocolpos, hematometra, hematosalpinx, endometriosis, and pelvic adhesions, so that reproductive performance is maintained.[6]
Whenever a genitourinary anomaly is suspected, an initial screening ultrasound of the pelvis and kidney, ureter, and bladder (KUB) should be done followed by MRI rather than computed tomography (CT) scan, as CT involves radiation exposure and has poor soft-tissue resolution. Considering the wide variations in uterovaginal anomalies, precise delineations of the uterus, fallopian tubes, cervix, and vagina are crucial. The status of these reproductive organs, the extent of endometriosis, and pelvic inflammation can be well evaluated with MRI.[8] Laparoscopy is the gold standard diagnostic modality with the additional advantages of therapeutic drainage of hematocolpos/hematometra and vaginal septectomy.[9,10] Vaginal septum excision is the treatment of choice for HWWS. Incidentally, in a study, it has been reported that successful pregnancy following surgical intervention was achieved in 87% of the patients, while 13% had the risk of abortion.[11]
CONCLUSION
The diagnosis of OHVIRA gets delayed due to vague abdominal symptoms in puberty. So strong suspicions and knowledge are essential for the diagnosis of this rare condition.
Early diagnosis of OHVIRA is crucial to prevent further complications like infertility and to maintain normal reproductive life, thus preventing marital disharmony and improving socioeconomic status.
USG of KUB and the pelvis is the ideal screening modality, whereas an abdominopelvic MRI is the imaging modality of choice.
Laparoscopy remains the gold standard not only for diagnosis but also for therapeutic options like drainage of hematocolpos, hematometra and hematosalpinx, excision of endometriosis, pelvic adhesiolysis, and vaginal septectomy.
Source of Support:
Nil
Conflicts of Interest:
None declared.
REFERENCES
- Uterus didelphys with obstructed hemivagina and multicystic dysplastic kidney. Eur J Pediatr Surg. 2005;15:441-5.
- [Google Scholar]
- Herlyn-Werner-Wunderlich syndrome consisting of uterine didelphys, obstructed hemivagina and ipsilateral renal agenesis in a newborn. Pediatr Neonatol. 2012;53:68-71.
- [Google Scholar]
- Müllerian anomalies: A proposed classification. (An analysis of 144 cases) Fertil Steril. 1979;32:40-6.
- [Google Scholar]
- A case of Herlyn-Werner-Wunderlich syndrome with recurrent hematopyometra. J Womens' Med. 2009;2:77-9.
- [Google Scholar]
- An unusual presentation of uterus didelphys with obstructed hemivagina with ipsilateral renal agenesis. Fertil Streril. 2008;90:849.e9-10.
- [Google Scholar]
- Uterus didelphys with unilateral distal vaginal agenesis and ipsilateral renal agenesis: Common presentation of an unusual variation. J Radiol Case Rep. 2011;5:1-8.
- [Google Scholar]
- OHVIRA syndrome (obstructed hemivagina and ipsilateral renal anomaly) with uterus didelphys, an unusual presentation. J Pediatr Adolesc Gynecol. 2012;25:e23-5.
- [Google Scholar]
- Uterus didelphys associated with obstructed hemivagina and ipsilateral renal agenesis: MR findings in seven cases. Abdom Imaging. 1998;23:437-41.
- [Google Scholar]
- Management and outcome of patients with combined vaginal septum, bifid uterus and ipsilateral renal agenesis (Herlyn-Werner-Wunderlich syndrome. J Pediatr Surg. 2006;41:987-92.
- [Google Scholar]
- Herlyn-Werner-Wunderlich Syndrome with unilateral hemivaginal obstruction, ipsilateral renal agenesis and contralateral renal thin GBM disease: A case report with radiological follow up. J Korean Soc Radiol. 2010;62:383-8.
- [Google Scholar]
- Double uterus, blind hemivagina, and ipsilateral renal agenesis: 36 cases and long-term follow-up. Obstet Gynecol. 1997;90:26-32.
- [Google Scholar]




